COVID-19 Predictions & Rampant Speculation: May 2020
It turns out that so far, I have written over 44000 words on COVID-19. I’ve tried very hard to only report the best and most trustworthy science, but I did strive to include interesting new insights that were not yet mainstream.
As an example, I spoke about vitamin D and sunlight real early, which now indeed appears to be a thing. No guarantees yet, but it definitely is a thing. I also mentioned the importance of ventilating indoor places early on, and this too now appears to be very relevant.
I have however not mentioned many other things because I understand that my role as a bystander is (at best) to explain or perhaps just popularize good science. I should not do my own speculation since there is so much armchair epidemiology going on already. In some posts I did include some clearly marked paragraphs with well labeled speculation.
However, it turns out I can’t hold it in. So here is a dumping ground of things I think I see emerging proof for, or things I expect to happen, or even just observations I want to share.
I’m listing this here to 1) up the chances that later on I can say “told you so” 2) as an exercise in intellectual honesty, because this forces me to write down my otherwise private & untested thoughts.
Also, what I really hate is when people describe a development as ‘predictable’ without ever having predicted it.
So here goes, big speculation, it might all be true, it might not be, but I have to vent!
NOTE: So this is very different from all my other corona posting, where I have tried very hard to objectively stick to the proven facts!
- Monoclonal antibodies (mabs) will be the first medicines that are truly COVID-19 gamechangers
- They will be relatively expensive, but will work for prevention and treatment.
- We will realize that even not too sensitive or specific antigenic rapid COVID-19 infection tests are very good at spotting infectious people. From a public health perspective we don’t care that much about missing non-infectious people.
- The combination of even not too precise rapid tests and early low-impact treatment might be exceptionally useful
- Sooner rather than later (“September”) there will be limited supplies of
not yet the best vaccines that have seen some real life testing, and no
one will know what to do with them
- Will they be good enough? And worth the risk of adverse events? Or should we hold out for better vaccines?
- Instead we may find “mabs” more interesting for temporary immunisation
- COVID-19 will be the breakthrough modern vaccine technologies (like mRNA) were waiting for, even should they fail to deliver the “best” vaccine in the short term. Their versatility might in turn mean great things for the flu shot & cancer medicine.
- In general, with some luck, COVID-19 will advance the state of molecular biology, virology and medicine as much as HIV did. Science has sped up tremendously already.
- For COVID-19, scientific journals temporarily moved to an open access
model. Normally, scientists submit papers for free, other scientists
review these papers for free, and we then all get to pay ridiculous
amounts of money to see these articles, which no one got paid for. This
is and was ridiculous and COVID-19 should be the end of it.
- Note that all conspiracy theories moved to open access long ago!
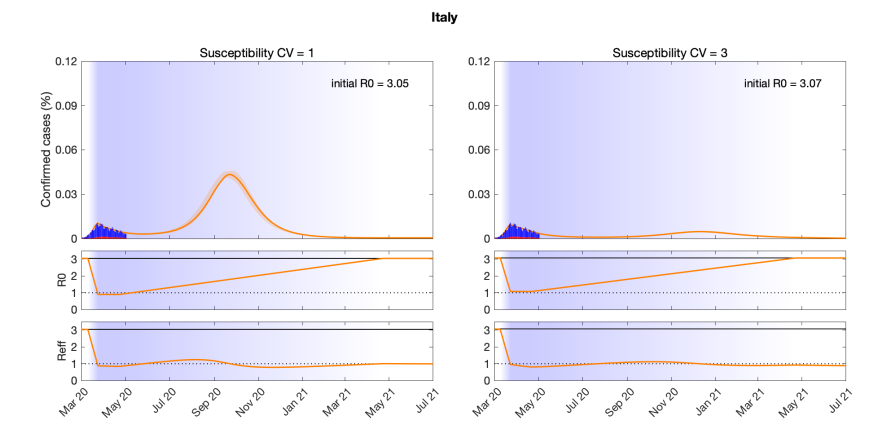
- Spread of COVID-19 will turn out to be heavily modulated by individual
variations in susceptibility. Many of us, between 20% and 70% I estimate,
are able to fend off reasonable doses of COVID-19, because of our innate
immune system, or remnant antibodies (or T cells) against the other 4 circulating corona
viruses.
- Added 6th of June, post on COVID 19: The T Cell Story
- Such variable susceptibility will likely in some places lead to “herd immunity levels” that are far far lower than the oft mentioned 66%, as discussed in R and the Herd, perhaps 20%, perhaps lower.
- I think this is part of the explanation why so many outbreaks are slowing down, even with populations (no longer) physical distancing very well. See also “overdispersion” below.
- My pet theory is that a light exposure to COVID-19 can lead to an
infection you don’t really notice (and that we can’t detect reliably),
but that still generates some immunity. I asked an actual
expert and
he said “maybe”.
- I wrote a bit about our amazing immune system
- “The R0 of COVID-19” is bunk. And that we chased it for months shows
that not only did the general public not understand the concept of R, whole
swathes of professionals did not do so either. And the ones that did
understand it (more power to them) did not get a voice.
- There is however the concept of R0 for a virus + a specific population + existing traffic patterns + prevailing weather conditions etc. R as a concept works, but it is not an aspect of the virus proper.
- I hate to say it, but most epidemiological models have not only been wrong but also not very useful. Only a very limited number of models incorporated variability of susceptibility and exposure, and no model I know of modeled both at the same time. As noted above, turns out this is important, and may explain why so many outbreaks are leveling off even despite very mediocre adherence to physical distancing rules.
- Computer scientists should generally not attempt to become epidemiologists overnight, even if they have read papers on SEIR models and have a Medium account.
- Epidemiologists should get their code peer reviewed by actual programmers
if they expect their models to be used for real decision making.
- Neil Ferguson has now been roasted sufficiently, so I won’t add to that, but the point stands.
- I’ll gladly volunteer to review any such code
- COVID-19 will upset our understanding of respiratory virus transmission and put it on a far more solid basis. It was ridiculous that going into this outbreak so many questions about SARS-CoV-1 & influenza were still unanswered.
- Political journalists should not cover science and health events. Send health and science journalists. Just try it for once, see what happens.
- Vitamin D history and sunlight exposure will turn out to have
mattered greatly for innate immune system performance, but this will
remain controversial.
- Sunlight may turn out to be more important than vitamin D per se.
- Note that vitamin D is never an easy story, but the signal for its causal effect on respiratory diseases in late winter is now quite solid.
- Air pollution that reduces UVB exposure will turn out to have been
very(update on 24th of May, removed ‘very’) important in the “summer before” (so “July 2019” for the northern hemisphere).- Look at the COVID-19 experience of countries coming “from” summer compared to those coming from winter and compare.
- Almost every country has a unique vitamin D and sunlight exposure profile, which makes comparisons very hard. Taiwanese elderly for example have sufficient vitamin D, while younger people don’t. The situation in The Netherlands is the exact reverse.
- COVID-19 spread is widely ‘overdispersed’, meaning that many people infect no one, and some others infect whole choirs. This is a “spark” transmission model where most sparks don’t cause a fire. The biggest effect of lock-down measures will have been to prevent sparks reaching large congregations of people (in offices, factories, public transport, churches).
- The extremely variable outcomes of epidemics between countries or even
regions in those countries will turn out to have been related to chance
events. Specifically, if any sparks “took”, or if several mass events
managed to infect each other.
- The eventual size of the epidemic is then likely the “overshoot”, where the epidemic rushes past where it would eventually end up with slower spread
- Countries that had limited outbreaks may be feeling smug, but they may just have been lucky
- Other countries clearly worked very hard on their well earned success
- Because of overdispersion lowering “herd immunity”, and the absence of
mass indoor events, northern hemisphere countries with somewhat
reasonable policies and populations will see their outbreaks die out over
the coming few months
- With lots of flare-ups related to specific events or workplaces
- If mass indoor events return and people do not fix their vitamin D
deficiencies, the virus will come back for a second general wave starting
November or December (northern hemisphere).
- Every country south of 40S is worth watching right now to see what happens as they move into winter
- Although the epidemic is subsiding in many places, which is great, be mindful of regions that saw extremely limited spread so far. They are “virgin ground” for flare ups again, much more so than those that went through an outbreak.
- There barely is any outdoors transmission and forcing people to stay indoors will be seen as a grave mistake
- Hospitals and healthcare settings will have been huge drivers of early parts of epidemics. This will be very controversial, but can you imagine a better hub of infection than an overfull waiting room, filled with people not feeling well where some of them have actual COVID-19?
- Singing will be found to not only spread virus particles very
efficiently, as yet uninfected singers will also inhale the virus deeply,
which will contribute to the pathology.
- “Talking loudly in a loud pub” might be a worst case scenario as well for similar reasons. A busy restaurant might work the same way.
Added 25th of May:
- Contact tracing / exposure notification apps will likely not turn out to be useful given spreading patterns. Instead, we may find it important to rapidly find people who were at gatherings that turned out to be a “super spreading event”
Thank you for making it to the end of this page! If I gain any new insights, or find that some of the things above turned out not to be true, I’ll make a note of this, but not remove my wrong predictions.
Added 31st of August:
I am not going to promote or link this piece since there is enough amateur speculation out there. But I do want to write it up to record my prediction and to keep me honest if I was wrong.
So in Europe we are seeing large increases in number of positive COVID-19 tests in countries like Germany, Belgium, The Netherlands, the United Kingdom, Luxembourg, Spain etc. But what we aren’t seeing is larger numbers of people dying or filling up ICU capacity.
In addition, at least in The Netherlands and Belgium, which both had serious first waves, it does not appear that this ‘second wave’ has legs (despite massive amounts of testing). In many places, the amount of positive tests is already going down again, and it is in any case not increasing in most regions.
An initial interpretation was that this second outbreak was hitting mostly younger people (which is true), and that these do not get severely ill at like anything the rate that older people do. This is indubitably true, but it doesn’t look like it is the whole story.
During Florida’s first wave, the infections started among younger people too, but they quickly infected their parents and grandparents, leading to significant amounts of death and severe disease. But we don’t see that happening here now.
So did anything change? Why is the epidemic behaving differently now here? We know the virus didn’t change (significantly) between the first and second waves.
I posit three possible reasons:
- Our behaviour is better. In a sense this is true, we’ve removed quite a lot of ‘superspreading potential’. But in other senses, it is sometimes hard here to see that an actual epidemic is going on. Streets, shops and restaurants are bustling.
- Everyone is now at peak vitamin D concentrations.
- And here is my pet theory: a lot of us have been exposed to some SARS-CoV-2 by now. And this may have primed our immune systems.
We don’t need a single explanation, it can be all three. So in terms of behaviour, it is now clear that COVID-19 has significant spread in indoor crowds under suitable conditions. Most people however do not manage to infect a single person, even among those they live with. But we do get these weddings where 50 people go home with the virus. So by preventing or limiting really large superspreading events, we are dealing the virus a big blow.
In terms of vitamin D, there continues to be a SHOCKING lack of research on this subject. It is well established that rectifying vitamin D deficiency helps prevent other respiratory diseases very well. But somehow we don’t think this is a priority for COVID-19. Each and every measurement on COVID-19 cases has found that patients with lower vitamin D status do way worse than people with adequate vitamin D levels. In August in the northern hemisphere, this should not be that much of an issue though, so perhaps we are seeing that too.
Lastly, there is my pet theory. So how do we get infected by a virus? Does it take one lucky virus particle? Or should a whole bunch of them arrive at the same time? Interestingly enough we don’t really know. There is the ‘independent action hypothesis’ which says every virus particle has a fresh chance of infecting a patient. Other research has shown that ‘hundreds, maybe a thousand’ virions are needed for an infection. But we really don’t know if it would work if these arrived sequentially over a few days, or if they have to arrive together etc.
It does look like getting an initial heavy dose of virus leads to worse outcomes.
So my pet theory is that if the region where you live has had an initial large wave, maybe 10% got infected for real, we can be sure almost everyone got exposed to some virus particles. The way our immune system works is that we have an innate immune system that generically fights threats, and it may often succeed in taming an infection, especially of the initial dose is small.
In addition to the innate immune system, our bodies literally evolve cells to deal with new infections, starting from templates that may or may not be a good fit already. This takes a week or ten days or so.
Now, my pet theory means that for everyone that got infected for real.. even more people had a sub-infective dose that nevertheless helped along the evolution of B and T cells. This means more suitable primers are now circulating.
If these people then encounter SARS-CoV-2 during the second wave, their outcomes may be very different from when a completely naive population was exposed for the first time during a first wave. Their immune systems still need to evolve B and T cells to counter the infection, but they aren’t starting from scratch.
Now, is this a plausible theory? It does have some things going for it. The way evolution works, it would be unlikely if our immune system did not evolve the ability to ‘sniff out’ new viruses that are circulating in low doses and learn from them already.
Beyond that, this theory can be used to predict that “second waves” will definitely be milder in terms of hospitalizations and deaths than first waves. And it also predicts that if a region of a country hasn’t had a significant first wave, it might get hit harder if a second wave does arrive.
Now, does this mean northern hemisphere winter will be fine? I think not. As long as people will become more vitamin D deficient and huddle closer together, we are offering the virus many new ways to circulate and stress out immune systems.