Vitamin D: the New COVID-19 Chloroquine?
Welcome to this post, in which we’ll be taking a trip through the wild and bumpy ride that has been Vitamin D & sunlight research over the past few decades, and what it might mean for COVID-19.
As with my previous post, before any non-specialist attempts to write something on COVID-19, we should wonder: are any actual experts already writing on this, and if not, why not. Enough badly informed stuff has already been published by amateurs that before posting we should be certain we are actually being helpful.
The world of vitamin D (and sunlight) is highly polarized, and many respected experts are wisely not wading in. Parts of the scientific world love vitamin D, significant parts find it quackery, while at the same time various professional dermatology bodies consider sunlight a proven carcinogen to be avoided at all costs, while other parts note that avoiding sunlight appears to be as deadly as smoking.
Even though we don’t have all the facts, as noted epidemiologist Marc Lipsitch notes in “Good science is good science”, during a pandemic we must work with what data we do have, and try to make the best decisions based on that.
In this post, I have attempted to summarise the “four poles” of vitamin D opinion as best as I could, and to come to a balanced conclusion. The reader should know that my personal bias is that vitamin D is playing a big role in COVID-19, but I hope that I have succeeded in giving all points of view a fair and neutral amount of attention.
Here is the very short summary of what I have found on COVID-19 and vitamin D:
- Take all measures you can not to be vitamin D deficient during this pandemic, in accordance with government guidelines. You can achieve this by supplementing vitamin D3 (2000-4000 IU/day), or getting sensible amounts of sunlight in summer months, where you should check public health advice and not just what dermatologists say.
6th of September UPDATE: A small-scale randomized control trial in Spain found that supplementing hospitalised COVID-19 patients with a vitamin D product kept almost everyone out of the intensive care unit. The trial is still a bit small, but in this very well balanced post by Chris Materjohn, we can read what it means. This only strenghtens the case not to become vitamin D deficient this fall/winter.
30th of May UPDATE: By a ratio of 2:1, reader feedback indicates the Internet feels I was not optimistic enough about vitamin D, despite my headline conclusion above. If you need some optimism, you can read about my personal biased feelings on Vitamin D and COVID-19. Further details can be found in this page by Karl Pfleger, Immediate eradication of inadequate vitamin D levels is needed. As a palate cleanser, I suggest then moving on to this massive 2014 systemic review which states “highly convincing evidence of a clear role of vitamin D does not exist for any outcome”, but also read this later more specific and positive review.
20th of May UPDATE: Various readers have rightfully pointed out you can’t just stock up on vitamin D3 and call it a day. You’ll also need a nutritionally complete diet that furnishes you with other vitamins and minerals. Vitamin D does not work in isolation! Note that this does not require you to only eat “health food”. Eggs, fish, cheese, liver and other glorious foods are also stuffed with nutrients.
Additional summary if you do not feel like reading thousands of words:
- Vitamin D is involved with many aspects of our immune system. Going into a COVID-19 infection vitamin D deficient is like going into battle without ammunition.
- In science, there is a vitamin D fanbase, which believes that if only we would rectify vitamin D shortages, our health would improve by bounds, and they are incredibly frustrated we are not doing this simple thing.
- To compensate, there is an even larger group (it appears) in medicine that thinks vitamin D only correlates with bad outcomes, and that fixing vitamin D will not actually be very helpful.
- Both of these groups make decent points!
- Vitamin D is generated by UVB radiation which in non-tropical zones is only available during summer, outdoors, and even then only for a few hours around noon. UVB intensity is also strongly influenced by air pollution.
- Vitamin D can also be supplemented, and many countries fortify staple foods, but sometimes with “the wrong kind of vitamin D”.
- Vitamin D is a stupendously difficult subject and many of its aspects have barely been researched. As an example, it is not clear what a healthy level of vitamin D is, nor how we apparently are able to sustain reasonable levels over winter.
- Lack of vitamin D is associated with “everything that is bad for you” (including “lack of money”, social economic status or deprived living conditions)
- Preliminary results show this is the case for COVID-19 as well, the association between bad outcomes and vitamin D status appears to be very strong, but it could still be a fluke.
- There is pretty strong evidence that supplementing vitamin D helps those who are deficient. For some reason a lot of trials have been done on people who weren’t particularly deficient, and supplementation does not help them (a lot).
- At highest risk of vitamin D shortage: people with dark skin living in non-equatorial regions, overweight/obese, sun avoiders, people who mostly work indoors, people living north/south of 40 degrees latitude, those who are pregnant or wearing veiled clothing.
- Average vitamin D levels do not tell us how deeply vitamin D plummets in winter time.
- Every country and region has a unique vitamin D situation. In Taiwan, the elderly have sufficient vitamin D, but younger people don’t. In The Netherlands this situation is reversed. This makes comparisons difficult.
- Although evidence is not as strong as we’d like it to be, no one in medicine would advocate fighting a COVID-19 infection while vitamin D deficient
- A healthy full body exposure to sunlight can generate 25000 IU of vitamin D in one sitting, without getting burned. 2000-4000 IU daily of D3 supplements will also work.
- Overweight and obese people need (far) more IUs to achieve the same effects.
The longer story
Recently, some researchers have posted statistics of Vitamin D concentrations measured in patients with severe or mild COVID-19 outcomes. Some of these statistics are, to put it mildly, spectacularly suggestive.
This has led to a Chloroquine-like surge of enthusiasm for vitamin D. Meanwhile, many eminent medical professionals have strongly indicated vitamin D is a sideshow and we should not be expecting any significant protection from it.
Vitamin D already had an active medical and non-medical fanbase, with adherents suggesting that proper vitamin D levels will stave off almost any disease. Meanwhile, many medical practitioners have taken the opposite position, that the vitamin is almost useless as a treatment target.
How can this be? And should we be stocking up on sunlight and/or vitamin D to keep us healthy and safe from COVID-19?
Vitamin D is a devilishly complicated vitamin, pre-hormone and medical marker. Many explainers take unwarranted shortcuts to make their point on the utility or futility of vitamin D. This page makes no such shortcuts and is therefore very long.
Some context
Vitamins are vital (hence the name) for our health. Unlike foodstuffs, our bodies don’t meaningfully “consume” vitamins: they just need to be there. Unlike proteins, fatty acids and carbohydrates, we don’t burn them for energy, nor do we (generally) use vitamins as building materials.
Vitamins range from very simple (like C) to highly complex (like B12). Vitamin D sits somewhere in between.
Like anything in nature, the story quickly gets complicated. Vitamins can do useful things on their own. As an example, vitamin C functions as an enzyme that aids in the production of neurotransmitters. Vitamin K is chemically required for the production of proteins that regulate the coagulation of blood.
Vitamins however can also be used to create signals which make cells do certain things. In this way a vitamin can also be a “pre-hormone”.
Practically speaking, vitamin D appears to have a role in maintaining endothelium integrity which is important during infections. There may also be other non-hormonal functions, but this has not been very well explored oddly enough.
What is well known is Vitamin D’s huge hormonal role: its hormonal form changes DNA transcription in many many ways. In other words, vitamin D is used to create a signal. In this way it regulates calcium and phosphates in our bodies, plus hundreds of other genes.
Because our bodies can make vitamin D using sunshine, some purists argue vitamin D isn’t a vitamin at all! Confusingly, other medical professionals say that vitamin D production by sunlight is “unreliable”, so we should see it as part of nutrition.
The eight kinds of vitamin D
Yes. And it turns out the details matter. For starters, there are two “trains” of Vitamin D molecules: D2 (plant and fungal origin) and D3 (animal origin). I will ignore D2 in this article, except to note that D2 and D3 are not interchangeable, and that D3 appears to be more potent and native for humans.
Under the influence of UVB light, animals convert an abundantly available precursor chemical into cholecalciferol. This precursor (7-dehydrocholesterol) is present in the skin or in wool.
Cholecalciferol is transported to the liver which converts it into calcifediol, also known as 25(OH)D. This process takes 7 days. Calcifediol circulates in blood, and when “vitamin D” gets measured, the 25(OH)D concentration is what is reported.
Calcifediol is described as “non-active vitamin D”, but this appears to be a misnomer. It is fair to say however that calcifediol is not a hormone.
Finally, the kidneys & parts of our immune system convert calfideiol into the actual hormone calcitriol, which pulls many levers in our genes and cells.
So, the chain is:
7-dehydrocholesterol + UVB -> cholecalciferol -> calcifediol -> calcitriol.
And, keep in mind this is all D3, there is a separate but similar D2 chain, but there the chemicals have ’ergo’ added to their names.
Ultraviolet light
As we climb ‘up’ the rainbow of light from red to violet, light particles (photons) get ever more powerful. No matter how much red light we shine on 7-dehydrocholesterol, it will never convert into (pre)vitamin D. It requires the considerable kick of an UVB photon to make it happen.
Ultraviolet light is a blessing and a curse in biology. The potency of UV light makes many chemical reactions happen that would otherwise never succeed. The downside is that UV light makes many chemical reactions succeed that we also very much do not want to occur!
As a prime example, a 260nm photon is very suitable for creating vitamin D, but is is also the frequency of light best absorbed by RNA and DNA, which might be damaged by it.
In this way, oddly enough, vitamin D production could in fact itself function as a form of ‘sunscreen’ to protect our DNA. This is theorized to be the billion year old origin of vitamin D.
It appears that nature has not only found a way to protect us against UV light but also to make good use of it.
Hormones
Nature uses chemicals to broadcast signals from one part of the organism to another. A very famous hormone is insulin, which is released from the pancreas, and causes cells to take up sugar. Some cells do so by stashing glucose as glycogen, other cells convert sugar into belly fat, all directed by insulin.
Another famous hormone is adrenalin, which is part of our fight-or-flight response. Melatonin is well known for broadcasting the ‘biological clock’, making sure all our cells have their watches synchronized.
Note: this being nature, nothing has one clear-cut function, and every hormone does several, sometimes conflicting, things at the same time.
To send a signal, an organism must release a hormone into circulation. A challenge is that making a hormone costs time, but it may be needed urgently. To deal with this, many hormones are kept “ready to serve” in an inactive state. Insulin for example is stored as crystals, ready to be released quickly if sugar spikes.
The hormonally active form of vitamin D is called calcitriol, and it is created from a non-hormonal form called calcifediol (or calcidiol). As calcifediol, it circulates in blood at dozens of nanograms per milliliter.
If the calcitriol hormone is required, our kidneys, macrophages (part of our immune system) and possibly other places, initiate the conversion from calcifediol. Interestingly, calcitriol circulates not at nanograms but at picograms per liter, perhaps at a 500-1000 times lower concentration than calcifediol.
Calcitriol breaks down relatively quickly, with a half-life of around 5-8 hours. This means our body can modulate the concentration of circulating vitamin D hormone with some reasonable time resolution.
The non-hormonal form is stable for weeks. One way to see it is that around 100 days worth of hormonal vitamin D levels could be generated from the non-hormonal circulation (all this within several factors of inaccuracy).
In this way, our blood might be seen to carry a “100 day stash” of vitamin D, but it appears the circulating form (calcifediol) breaks down with a half-life of perhaps two weeks.
It is unclear how our bodies generally succeed at maintaining reasonable vitamin D levels over winter. There is very recent evidence vitamin D shuttles in and out of our muscles in complicated ways.
Adipose tissue (“belly fat”) appears to absorb but not release vitamin D. If we want to do some armchair hypothesizing, perhaps people historically used to lose weight in winter, which definitely would release the stored vitamin D just when it was needed.
What vitamin D does
Typical descriptions read that vitamin D regulates calcium and phosphorus and influences over 200 genes. In addition, we’ve recently learned that vitamin D is used in our immune system, specifically to regulate the intensity of immune responses. Supplementing vitamin D clearly changes these responses.
Severe COVID-19 disease is typified by ‘cytokine storms’ which are seen as immune system overreactions, and such (over)reactions are regulated by vitamin D.
Very recently it has been discovered that macrophages, white blood cells that engulf (’eat’) unwelcome intruders, can form their own calcitriol from circulating 25(OH)D and use this to influence local immune system behaviour.
Even though the mechanisms behind all this are not yet clear, it seems eminently reasonable to assume that our immune system needs vitamin D to function well.
Vitamin D as a cure for disease
Here is what we know for sure. Low vitamin D levels in children cause a very nasty disease called rickets. According to research in children, any 25(OH)D level below 90 nmol/L in children is a good predictor of rickets.
It is also known absolutely for sure that vitamin D supplementation, or exposure to light with sufficient UVB cures and prevents rickets.
In addition, while rickets had nearly disappeared from most developed countries, it has recently made a return in the United Kingdom and likely in other countries as well. This may be indicative that our vitamin D situation is not good.
Very interestingly, a lot of studies have been done on vitamin D in ruminant animals, and these have provided strong data to support supplementation.
“Vitamin D levels”
Now we start to get to the meat of the discussion. In practice, when people say they measure vitamin D levels, they mean calcifediol levels (also known as 25(OH)D). This is the ‘stored’ form of the vitamin, often denoted as ‘inactive’. This last bit might be inaccurate, but it is fair to say calcifediol in any case is the non-hormonal version of vitamin D.
Calcifediol levels respond quickly and durably to exposure to sunlight containing UVB. Interestingly, calcifediol levels remain elevated longer from natural sunlight than after ingesting D3 from food or supplements.
Now, if we measure 25(OH)D levels in people, we quickly find that low “vitamin D” levels correlate with like everything bad. This includes cancer, heart disease, diabetes (all types), MS, depression, Parkinson’s, and Alzheimer’s. People with low vitamin D are doing a lot worse at everything. You’ll probably find that vitamin D correlates with stubbed toes too.
Such stonking data leads to theorizing of course, and a very plausible and simple theory fits these observations. Since modern people spend most of our time indoors, and have heeded government warnings to avoid the sun, most of us are at severe risk of low vitamin D status, especially late in winter. The theory then goes that if we just fix the low vitamin D status, tons of health problems will magically go away. This would be the biggest change in health in centuries.
“Explanations exist; they have existed for all time; there is always a well-known solution to every human problem — neat, plausible, and wrong” - H.L. Mencken
Not only is this theory plausible, it fits in with biases many of us hold, that being out in nature is good, being cooped up in buildings is bad and that slathering yourself in chemicals (sunscreen) is likely a bad thing. You can also add a dollop of armchair evolution theory to it - that sunlight is actually fine if you live where your genes evolved and have appropriate genetics for your climate, unlike say lily white people of English descent moving to the tropics. It is all very paleo.
The appeal of the theory is huge. And honestly, it is a very good hypothesis. It need not be true, but it desperately needs to be tested vigorously - the payoff would be tremendous. But we should be aware that this is a theory that many of us “want to believe”. This does not make it true.
Alternate theories
Now, while we should be careful not to fall in love with a theory to the extent that it blinds us to the possibility it might not be true, the reverse also holds.
There is a strange bias in many medical circles that vitamins are bunk. An unshakable conviction that we can and should get all our micronutrients from “normal food” - no matter how dire the ultra-processed food is that people actually can buy. The belief in the health effects of available food is rather touching - even when no common food contains significant amounts of vitamin D.
From such a position, there are a lot of ways to argue against the theory that vitamin D shortage is behind everything that ails us. The simplest attack on the hypothesis is that vitamin D status is actually a way of measuring social economic status. People who work shifts in factories and/or have no garden rarely get outdoors, so they won’t produce any vitamin D. People that take exercise outdoors are also naturally more exposed to sunlight, so vitamin D status might simply measure if people are exercising. The exercise might explain the positive effects, not the vitamin D.
One very good way of raising vitamin D levels is to go on a sunny holiday during autumn or winter - which highly correlates with wealth, which in turn correlates strongly with health.
Vitamin D status also correlates with fish consumption, which is notably higher among well educated people with time and inclination to cook. Then there is the so called “healthy user bias” - people already caring about their health might have been taking supplements, but these are clearly people interested in taking better care of themselves. Of course they do better!
There is also the inverse theory - it is not the lack of vitamin D that causes disease, it is disease that causes our bodies to somehow lose or use up vitamin D.
Another theory is that sunlight is actually good in moderate doses, far beyond just raising vitamin D levels. Vitamin D might simply be a marker for how much sunlight someone receives.
So, there are many reasons why vitamin D might be low in people with more disease burden, without low vitamin D actually being the causative agent.
This is summed up as ‘Vitamin D is not a maker of health but a marker of health’.
We need to take these arguments seriously.
Trials
Whenever there is doubt in medical circles, calls are made to perform Randomized Control Trials (RCTs). This is where we take matched (“equivalent”) groups, apply some form of treatment to specific groups, and not to other groups. Before we start the trial we state what outcome we are going to compare the groups on, and then we start the experiment. Extra bonus points for (double) blinding, so when participants and/or experimenters do not know which group someone is in.
In theory, an RCT can settle any question, but it might take a great amount of time, time we sometimes don’t have. There are sadly however many practical ways in which an RCT might not give you a useful answer.
Most RCTs on vitamin D supplementation have not given clear results either way so far.
Although science attempts to be impartial, every group of scientists I know starts their experiments because they hope to get a certain outcome. They run the RCT to get proof for their theories (or perhaps super convincing proof against their theories). This is ok as long as this bias is acknowledged, and if we are sure the RCT is designed well.
This last part is important. An RCT can for example be underpowered. I wrote a piece on this earlier. In short, small trials can be blind to even very large effects of a treatment. Let’s say 50 older people are treated and 50 are not. Based on previous experience, over a year, we might expect to see 5 cases of flu develop in an untreated group.
And lo, the outcome is that the untreated group had 4 cases of flu and the treated group had 6. Bring out the press releases, vitamin D doesn’t work!
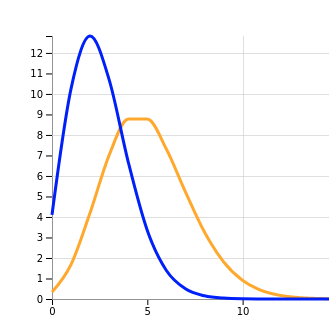
Here is a graph predicting outcomes in both groups even if we assume vitamin D supplementation would prevent half of all flu episodes.
On the x-axis is the number flu episodes in both groups, on the y-axis is the probability of that outcome.
From the huge overlap we can see that almost any outcome is possible under this scenario. This RCT would never have taught us anything, even if no one fell ill in the treatment group we would not be very sure that vitamin D made a difference.
I tell this longwinded story because the outcome of even such an underpowered an RCT is frequently heralded as “settling the science”, when this is not the case.
Bickering over RCT design
If an RCT does not deliver the expected result, a standard toolkit is deployed to cast doubt:
- The treatment was not strong enough
- The treatment was not long enough
- They actually used the wrong treatment
- They actually used incomplete treatment
- The experiment was underpowered
- Patients did not adhere to the treatment
- The wrong outcome was measured
- The patients were the wrong ones
As examples, of all these:
- 1000 IU/daily of vitamin D is not enough
- Damage of low vitamin D status builds up, you can’t do a 4 month trial and expect results
- Vitamin D3 should be used and not D2
- The study group was malnourished in other ways as well, which were not addressed
- Underpowered: see above
- People hate taking pills daily, you did not check if participants actually complied
- You measured flu incidence but not intensity of disease
- Testing vitamin D supplementation on people that are not vitamin D deficient
It should be noted that if 20% of the population has a vitamin D deficit, any supplementation trial on random people will struggle to show a benefit, even if disease is entirely eliminated from that 20%.
Despite dozens of RCTs on vitamin D, there haven’t been many very good ones. Or in other words, almost any RCT that has shown an effect can be criticized (too small, too selective), as can almost any RCT that showed a disappointing effect.
So far only a few things are clear:
- Vitamin D supplementation is not some kind of miracle cure for everything in the short term
- Vitamin D supplementation is very safe
- There have been a few hard to discount very positive RCTs and a positive systemic review of the effect of supplementation on respiratory tract infections in vitamin D deficient people.
To extract a clear signal, an RCT might recruit participants with low vitamin D status in early summer, initiate supplementation and measure health outcomes during winter.
A bit on sunlight
Vitamin D levels in the UK fluctuate by 50% over the year:
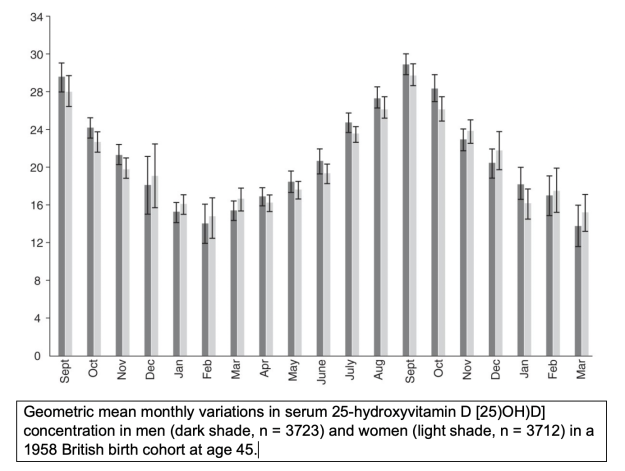
Someone who is not deficient late summer stands a good chance to be deficient at the end of winter, when levels have halved.
Regular exposure to sunlight also appears to be robustly associated with better health. This might be for many reasons, and vitamin D generation is plausibly one of them.
Now, through years of hectoring by dermatologists, many of us now assume that sunlight is something to be avoided, by not going into it, by covering up or ‘slip slop slapping’ ourselves with sunscreen.
From a dermatologist perspective, any case of skin cancer is one too many of course. And strictly speaking, since we know that getting sun burned is very harmful, it is possible to state that “sunlight is a proven carcinogen”.
Excessive sunlight can indeed be harmful, especially in regions and populations (Australia, for example) where there is significant mismatch between skin color and solar strength. The inverse effect is observed when dark skinned people live in the Nordics, where they typically become vitamin D deficient.
Although excessive sunlight is definitely harmful, it appears that the same goes for insufficient exposure to sunlight. There is research that shows that for Swedish women, avoidance of sunlight is associated with the same risks as smoking, for example. The optimal dose of direct sunshine exposure is not zero, despite what some professional bodies claim.
The situation is highly emotional. The word ‘cancer’ inflames opinions, it is the atomic bomb of arguments. Especially if someone has personally had a scary diagnosis.
National public health organizations have to weigh all the evidence, including that from dermatologists but also many other medical specialisms.
The Dutch health council for example states the following on sunlight:
We advise a daily exposure to sunlight of at least 15 to 30 minutes, between 11AM and 3PM, when the sun is high in the sky, with uncovered head and hands.
Now, this is advice for a somewhat northerly country (53N), but this is the outcome when they weigh all the evidence.
A good discussion can be found in Sun Exposure Public Health Directives.
I realize that for some people every ray of sunlight will be considered as harmful, but based on all the evidence, this is far from the case.
On balance
What to make of this situation? It seems clear no one should be vitamin D deficient, and no medical professional will argue for trying to fight COVID-19 while being deficient in anything useful.
The RCTs clearly show that vitamin D is not a miracle cure for everything, but simultaneously, many RCTs have design issues that make their outcomes less than convincing. And there have been some very positive ones.
We are left with the observation that people with bad vitamin D status do worse on nearly everything, and appear to have very bad COVID-19 outcomes. This observation is biologically very plausible, especially given the cytokine storm observations.
The Bradford Hill criteria for causation list strength, consistency, biological gradient, plausibility and experimental evidence as indicators for when correlation might imply causation, and all these are met by the COVID-19 observations so far.
At minimum we can therefore conclude that we can safely urge people to take steps to make sure they are not vitamin D deficient, and also not to be so once winter arrives. I think it is impossible to argue that this is bad advice, and there are a lot of reasons to think it will help.
Speculation
Given what I have read, I would not rule out that vitamin D generated from actual sunlight might be more beneficial, but proof is very thin. It is now known that sunlight enables other chemical reactions beyond synthesizing vitamin D, and some of these influence our immune system.
It is tempting to look for epidemiological evidence for the role of vitamin D in COVID-19. If we look at countries that had stronger or more moderate outbreaks, I think we can see a vitamin D influenced pattern, but good data is hard to find. We don’t just need to know “average vitamin D levels”, but specifically we must have the distribution of levels in February, March and April. Also, the outcome of an outbreak is of course influenced by people’s behaviour, government policy and many other things as well. This clouds the signal.
We can also speculate a bit why some outbreaks in the Northern Hemisphere are dying down so rapidly and show no sign so far of flaring up again. Might returning to healthier “spring” vitamin D levels be playing a role in keeping the epidemic small?
And might the diversity of vitamin D statuses have contributed to variations in COVID-19 susceptibility? Such variable susceptibility has been suggested to help stem the epidemic even before full “herd immunity” is reached, as noted in my previous post.
Further reading
Up to date site providing links to evidence:
Here are various links I used to prepare this post:
https://nutrition.bmj.com/content/early/2020/05/20/bmjnph-2020-000096 - Avoidance of vitamin D deficiency to slow the COVID-19 pandemic
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3941824/ - bioavailability of vitamin D
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6776467/ - The Role of Skeletal Muscle in Maintaining Vitamin D Status in Winter
https://sci-hub.tw/10.1210/jc.2017-01187 - Martinaityte, I., Kamycheva, E., Didriksen, A., Jakobsen, J., & Jorde, R. (2017). Vitamin D Stored in Fat Tissue During a 5-Year Intervention Affects Serum 25-Hydroxyvitamin D Levels the Following Year. The Journal of Clinical Endocrinology & Metabolism, 102(10), 3731–3738. doi:10.1210/jc.2017-01187
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6365669/ - Vitamin D testing and treatment: a narrative review of current evidence
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6425757/ - Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6121423/ - Vitamin D and Influenza—Prevention or Therapy?
https://www.sciencedirect.com/science/article/pii/S1871402120301156?via%3Dihub - association with vitamin d and covid-19 diagnosis
https://www.dsm.com/markets/anh/en_US/Compendium/ruminants/vitamin_D.html - this is a surprisingly good read on vitamin D for cows. Veterinarians have far fewer hangups and are far more pragmatic on preventing disease.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2835877/ - The possible roles of solar ultraviolet-B radiation and vitamin D in reducing case-fatality rates from the 1918–1919 influenza pandemic in the United States
https://www.bmj.com/content/356/bmj.i6583 - Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data (showing it works on vitamin D deficient people).